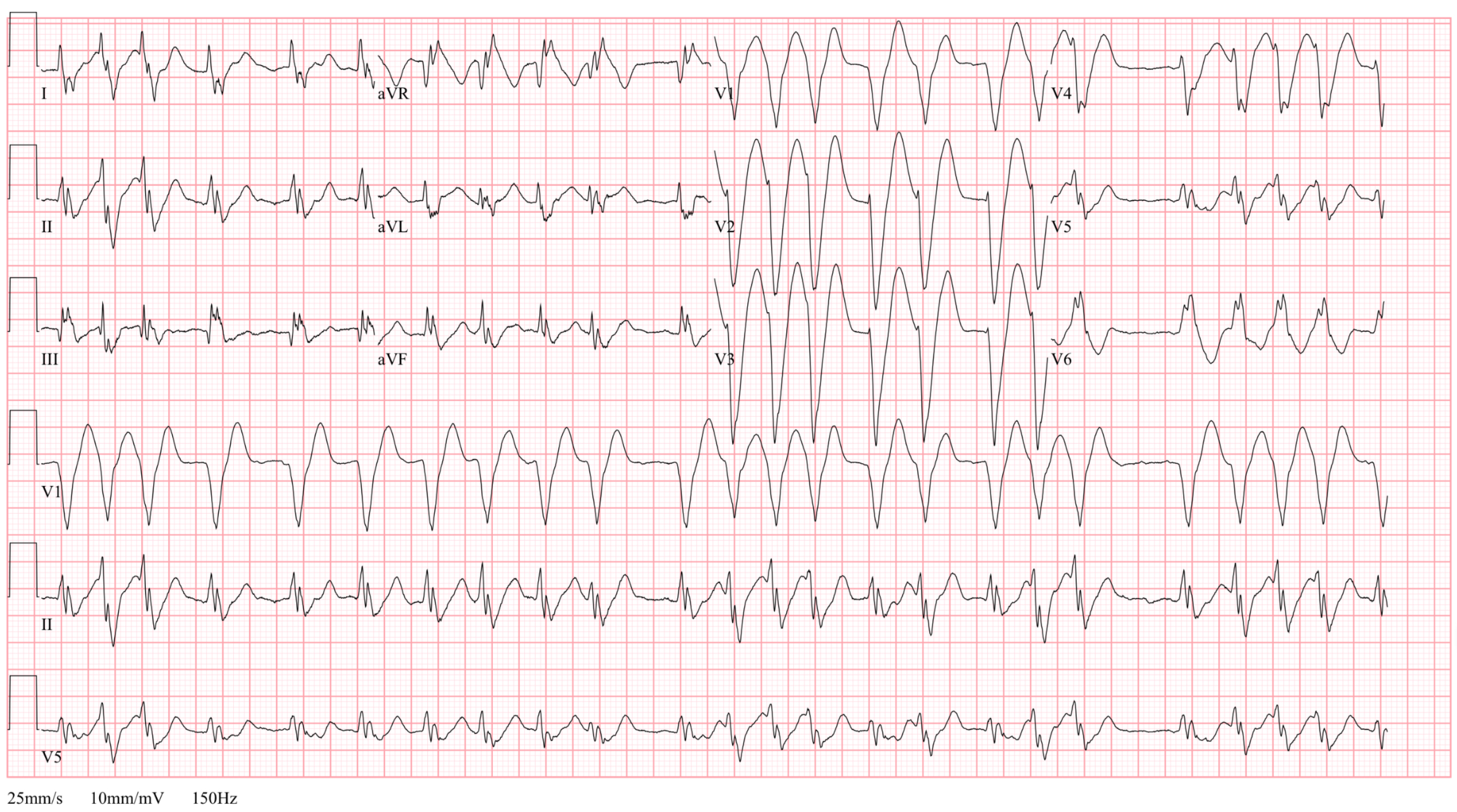
This patient presented with palpitations. Their blood pressure was good and they were alert and talking. They had a strong preference not to be shocked. What is this EKG and what drug would you use to treat it. Hint: the QTc = 580 ms. There is no old EKG.
Answer
The EKG shows a monomorphic, irregular ventricular tachycardia in a stable patient. The safest treatment modality is cardioversion. In this case, the patient preferred not to be shocked. We were also unsure about the time frame of the a fib so had to worry about an atrial thrombus. There were also several features that potentially limited drug choices:
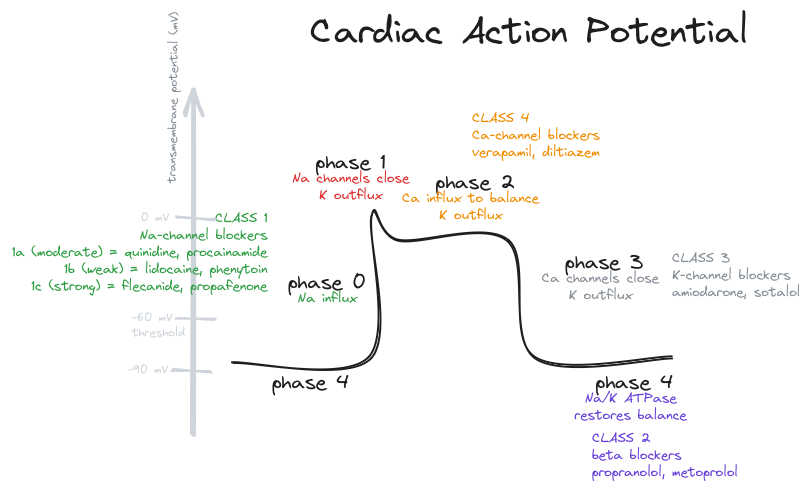
- The wide QTc pushed us from Class I drugs which may further prolong it:
procainamideandamiodarone - With wide irregular rhythms you need to consider aberrancy (eg, WPW) so AV nodal blockers could have been dangerous:
metoprolol, diltiazem, adenosine and digoxin - We weren’t considering a toxicologic cause, but if we were we should avoid other Na-channel blockers.
Ultimately, in discussion with EP Cardiology, we decided to go with a beta-blocker seeing as there was no visible delta wave. The heart rate slowed down quite nicely and the patient went for an ablation the next day.
From a recent EMRAP episode in June
Stable, monomorphic ventricular tachycardia

- Procainamide is the agent of choice, faster and more effective than procainamide
- Amiodarone is a reasonable second-line drug. It’s a class I, II, III and IV (pretty good at a lot of things but not the best at anything).
- Do not use either in patients with prolonged QT.
…with prolonged QTc
- Electricity is preferred due to potential complications from the QT prolongation
- AVOID: procainamide (Class 1A) and amiodarone (Class IA effects) as they can worsen dysrhythmias with underlying prolonged QT.
- Lidocaine is a reasonable first-line choice even though it’s a Na-channel blocker, it doesn’t seem to prolong the QT that much.
- Magnesium can be given as well.
- Beta-blockers and CCB might be okay as long as the wide complex isn’t due to an accessory pathway
…with Brugada syndrome
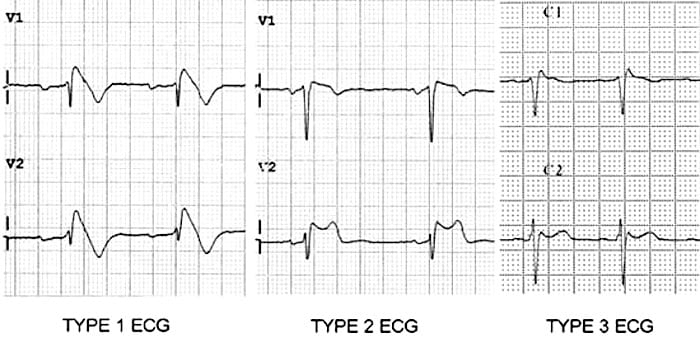
- Brugada is due to a sodium channel defect from one of many genetic mutations.
- Type 1 has > 2mm of STE and a coved ST segment
- Type 2 has > 2mm of STE and a saddleback deformity
- Type 3 has < 2mm of STE but the shape of type 1 or 2
- Avoid sodium channnel blockers. Stay away from lidocaine, amiodarone, procainamide.
- Brugada will deteriorate into VT. You’d need an old EKG to see the prior Brugada.
- Isoproterenol (Class IIa) is the chemical agent of choice.
…with atrial fibrillation
- The worry with wide complex atrial fibrillation is an underlying WPW. Usually this is a morphology-changing QRS, rates > 200 and normal axis. VT can have strange axes.
- Electrical cardioversion is preferred, but avoid AV nodal blockers.
